Imagine your heart as a high-performance engine. For it to keep running, it needs a constant supply of fuel and oxygen, delivered through a network of specialized pipes called coronary arteries. But what happens when those pipes get clogged? That is exactly what happens with Coronary Artery Disease is a condition where the major blood vessels supplying the heart become narrowed or blocked. It is not something that happens overnight; it is a slow, silent build-up that can eventually lead to a heart attack if left unchecked. According to data from the World Health Organization, ischemic heart disease-the clinical term for this process-was responsible for roughly 13% of all global deaths between 2000 and 2021.
The Silent Build-Up: What is Atherosclerosis?
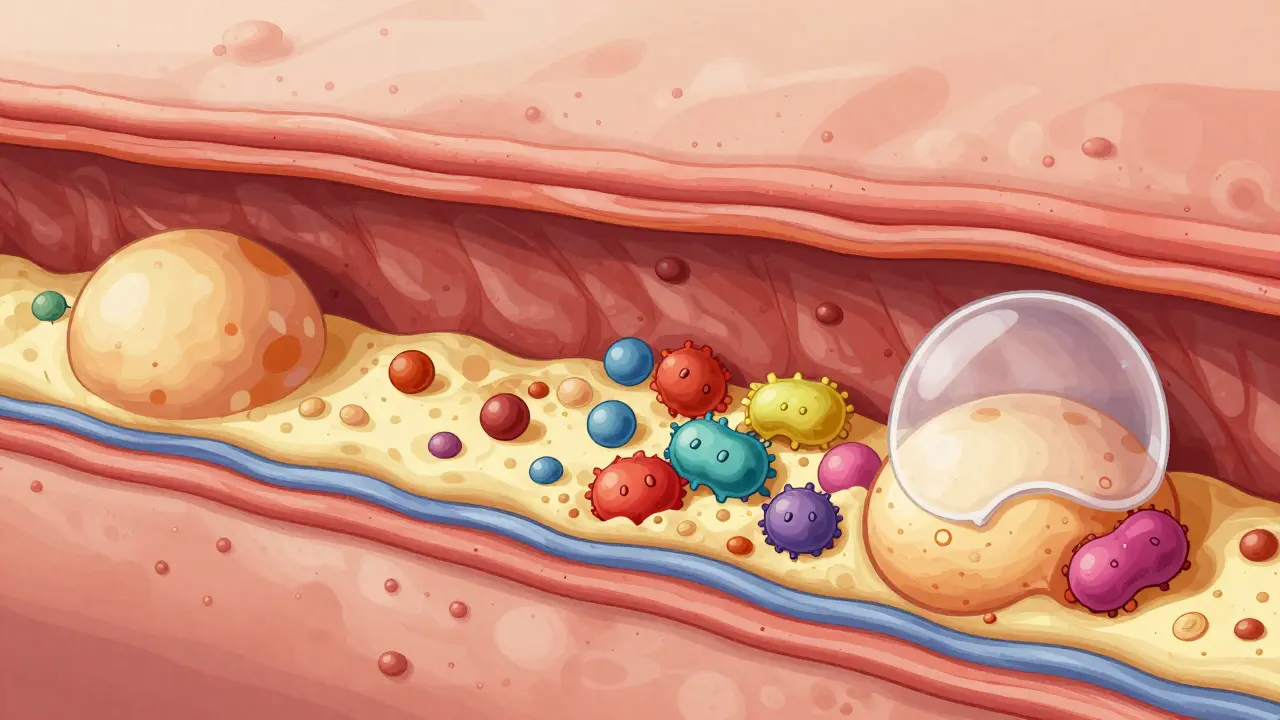
To understand heart disease, you have to understand Atherosclerosis. Think of it as "hardening of the arteries." It starts when the inner lining of your artery gets damaged. This damage allows LDL (the "bad" cholesterol) to seep into the wall. Your immune system tries to clean it up, but the cells that do the cleaning-macrophages-get stuck and turn into fatty streaks.
Over time, this mixture of fat, cholesterol, and calcium forms a plaque. Now, here is the part that surprises most people: not all plaques are the same. You might have a "stable" plaque that slowly narrows the artery by more than 50%. This usually causes predictable chest pain during exercise because the heart isn't getting enough blood. Then, there are "unstable" plaques. These might only narrow the artery by a small amount, but they have a thin, fragile cap. If that cap ruptures, it triggers a blood clot that can instantly block the artery, causing a heart attack. This is why a "mild" blockage can sometimes be more dangerous than a severe one.
Who is at Risk? Identifying the Red Flags
Not everyone develops heart disease, but certain factors significantly tilt the odds. Doctors generally categorize patients into low, intermediate, and high-risk groups. If you have a yearly risk of a cardiovascular event higher than 3%, you're in the high-risk category. But how do you know if you're heading that way?
Some risks are things you can't change, like your age or family history. Others are lifestyle-driven. Common red flags include:
- High BMI: Carrying excess weight puts a mechanical and metabolic strain on the heart.
- Diabetes: High blood sugar levels damage the arterial walls, making it easier for plaques to form.
- Dyslipidemia: This is a fancy way of saying your cholesterol levels are out of whack-usually too much LDL and not enough HDL (the "good" cholesterol).
- Hypertension: High blood pressure acts like a pressure washer inside your arteries, creating micro-tears that attract plaque.
- Smoking: Chemicals in cigarettes damage the endothelium (the artery lining) and make blood more likely to clot.
Interestingly, the medical community is seeing more cases of "co-morbidity." For example, the field of cardio-oncology has emerged because as cancer survival rates improve, doctors are finding that patients are living long enough to develop chronic coronary disease, requiring a very delicate balance of treatments.
| Feature | Stable Plaque | Unstable Plaque |
|---|---|---|
| Fibrous Cap | Thick and strong | Thin and fragile |
| Lipid Core | Smaller | Large, fatty core |
| Vessel Narrowing | Typically > 50% | Often < 50% |
| Primary Symptom | Predictable chest pain (Angina) | Sudden blockage (Heart Attack) |
How Doctors Find the Blockage
If you're feeling shortness of breath or a tightness in your chest, your doctor won't just guess. They use a tiered approach to see what's happening inside your chest. Usually, it starts with an Electrocardiogram (ECG), which records the electrical activity of your heart to see if there are signs of a past or current heart attack.
If the ECG isn't clear, they might suggest a stress test. This involves putting you on a treadmill or using medication to make your heart work harder. When the heart is under stress, any area that isn't getting enough blood becomes obvious on the monitor. For a definitive look, doctors use Coronary Angiography. This is an invasive procedure where a contrast dye is injected into the arteries and viewed under X-ray. It's essentially a map that tells the surgeon exactly where the blockages are and how severe they are.
For those who also have issues with blood flow in their legs, doctors often use the Ankle-Brachial Index (ABI). By comparing the blood pressure in your ankle to the pressure in your arm, they can diagnose Peripheral Artery Disease, which almost always goes hand-in-hand with heart disease.
Treating the Disease: From Lifestyle to Surgery
The goal of treating heart disease is twofold: stop the plaques from growing and prevent a total blockage. This is usually handled through a combination of "conservative" and "interventional" methods.
Lifestyle and Medication
First, you tackle the root causes. This means a heart-healthy diet (think Mediterranean style-lots of olive oil, fish, and greens) and regular movement. On the medication side, doctors often prescribe statins to lower LDL cholesterol and blood pressure medications to reduce the strain on the arterial walls. If you've already had a heart attack, you'll likely be on antiplatelet therapy for life to keep your blood from clotting around a plaque.
Interventional Procedures
When lifestyle changes aren't enough, doctors move to physical interventions. One common method is Percutaneous Coronary Intervention (PCI). During this procedure, a tiny balloon is inflated to push the plaque against the artery wall (angioplasty), and a small mesh tube called a stent is left behind to keep the artery open.
For more complex cases-like when multiple arteries are blocked or the blockage is in a critical location-surgery is the best bet. Coronary Artery Bypass Grafting (CABG) involves taking a healthy blood vessel from another part of the body (like the leg or chest) and sewing it around the blockage. It's essentially building a detour for the blood to flow around the traffic jam.

Managing Your Long-Term Heart Health
Living with heart disease is a marathon, not a sprint. Many people assume that once a stent is placed, the problem is solved. That's a dangerous misconception. A stent opens one spot, but it doesn't cure the underlying atherosclerosis. The rest of your arteries are still susceptible to plaque build-up.
The modern approach to care is highly personalized. Doctors now use a risk-stratification system to decide how aggressive the treatment should be. If you have heart failure or kidney disease (low eGFR), you're considered high-risk, and your medication and monitoring will be much more intense. The key is consistent follow-up. Your needs today might be different from your needs in two years, and dosages for blood thinners or cholesterol meds often need tweaking based on your clinical response.
Can atherosclerosis be reversed?
While you cannot completely "erase" old, calcified plaques, you can stabilize them. Through aggressive LDL lowering (usually with statins) and lifestyle changes, the plaques become denser and less likely to rupture, which significantly reduces the risk of a heart attack.
What is the difference between stable and unstable angina?
Stable angina is predictable; it happens during exertion and goes away with rest. It's caused by a narrowing of the artery. Unstable angina is unpredictable, can happen at rest, and is often a warning sign that a plaque has ruptured and a clot is forming. This is a medical emergency.
Does a stent last forever?
Stents are designed to be permanent, but the artery can sometimes narrow again inside the stent (called in-stent restenosis). This is why lifelong medication, like aspirin or other antiplatelets, is required to prevent clots from forming on the stent's surface.
How do diabetes and heart disease relate?
Diabetes causes high blood glucose, which damages the endothelium (the inner lining of arteries). This damage makes it much easier for fats and cholesterol to penetrate the artery wall, accelerating the process of atherosclerosis.
Is CABG surgery always better than a stent?
Not necessarily. PCI (stents) is less invasive and has a quicker recovery time, making it ideal for single-vessel disease. CABG is generally preferred for "multi-vessel disease" or when the left main coronary artery is blocked, as it provides a more durable long-term solution for complex blockages.
Next Steps for Heart Health
If you're worried about your heart, start with the basics. Get your blood pressure and cholesterol checked-these are the two most important numbers for predicting risk. If you have a family history of early heart attacks, ask your doctor about a calcium score test or an advanced lipid panel to see if you have high levels of Lipoprotein(a), a genetic risk factor.
For those already diagnosed, the most important thing is adherence. Skipping a statin or an antiplatelet pill for a few days might not seem like a big deal, but it removes the "chemical shield" that keeps your plaques stable. Work with your healthcare provider to create a personalized plan that accounts for your specific risk category, whether you are low, intermediate, or high risk.


Valorie Darling, April 20, 2026
everyone knows the mediterranean diet is basically just a trend anyway’
Shalika Jain, April 20, 2026
Please. The obsession with the 'Mediterranean diet' is so quaintly middle-class. In India, we have an entire spectrum of heart-healthy fats that the Western medical industrial complex completely ignores because it doesn't fit their narrow, Eurocentric paradigm of 'wellness'. It's honestly laughable how we just default to olive oil as the gold standard when the biochemical markers for lipid stabilization are far more nuanced than a few fancy salads and some grilled fish. I've seen far more sophisticated approaches to cardiovascular health in traditional Ayurvedic practice than what is presented in these basic summaries.
Brigid Prosser, April 20, 2026
Spot on with the plaque stabilization part. It's like patching a leaky dam rather than pretending the water isn't there. People get way too complacent after a stent, thinking they've got a magic fix, but the systemic inflammation is still simmering in the background.
Aaron McGrath, April 21, 2026
LISTEN UP!! You cannot ignore the endothelial dysfunction here! If you aren't aggressively targeting your LDL-C and ApoB levels, you're basically just waiting for a myocardial infarction to happen! Stop playing around with 'moderate' changes and start hitting the gym and optimizing your biomarkers NOW!! Get that blood flow maximized or you're just failing your own heart!!
Mike Beattie, April 22, 2026
The discourse here is lacking a certain clinical rigor regarding the hemodynamic instability of thin-cap fibroatheromas. Most of you are speaking in layman's terms while ignoring the actual pathophysiological cascade. The sheer negligence in managing the eGFR-cardiovascular nexus is palpable in these comments. It's a classic case of cognitive dissonance where people believe a lifestyle tweak can override a genetic predisposition toward hyperlipidemia. Truly exhausting to witness such a lack of biochemical understanding.
Lynn Smith, April 23, 2026
I totally agree with the point about the chemical shield! It's so important to stay on those meds.
Arthur Luke, April 24, 2026
The distinction between the stable and unstable plaques is a very helpful way to visualize why some people have a heart attack despite having relatively clear arteries on a previous screen. It really highlights the volatility of the disease.
Grace Grace, April 24, 2026
Oh my goodness!! Please please pleaze don't skip your statins!! It is so terrifying to think about a rupture happening just because someone wanted to save money on a prescription!! You guys have to be so careful with your health!!
Don Drapper, April 25, 2026
The sheer audacity of assuming that a basic dietary change could mitigate the profound systemic failure of an aging cardiovascular system is an absolute tragedy of ignorance. We are discussing the catastrophic collapse of arterial integrity, yet the responses are filled with a banal optimism that is frankly offensive to anyone with a rudimentary understanding of pathology. This is an exercise in futility.
Akshata Kembhavi, April 26, 2026
I think it's really nice how this explains everything so simply for people who aren't doctors.
Lucy Kuo, April 27, 2026
It is truly an honor to see such a comprehensive overview of these cardiovascular challenges. One must emphasize the profound necessity of compassion for those navigating the complexities of co-morbidity, especially those battling cancer while managing their heart health. It is a heartbreakingly delicate balance that requires the utmost grace and precision from the medical community. We must ensure that no patient feels abandoned in the shadow of such daunting diagnoses.
caesar simpkins, April 29, 2026
Man, that part about the pressure washer inside the arteries really paints a picture. Just absolutely wild how something you can't feel for years just destroys the pipes from the inside out. Truly a silent killer.
aman motamedi, May 1, 2026
I find the information regarding the Ankle-Brachial Index to be quite illuminating and relevant.
Charlotte Boychuk, May 1, 2026
This whole thing is just a whirlwind of scary stuff but the part about stabilizing plaques is a little ray of sunshine, isn't it? Just keep those levels low and keep the vibes positive and the heart pumping!
It's all about finding that sweet spot where you're healthy but not stressing yourself into a panic over every single heartbeat.