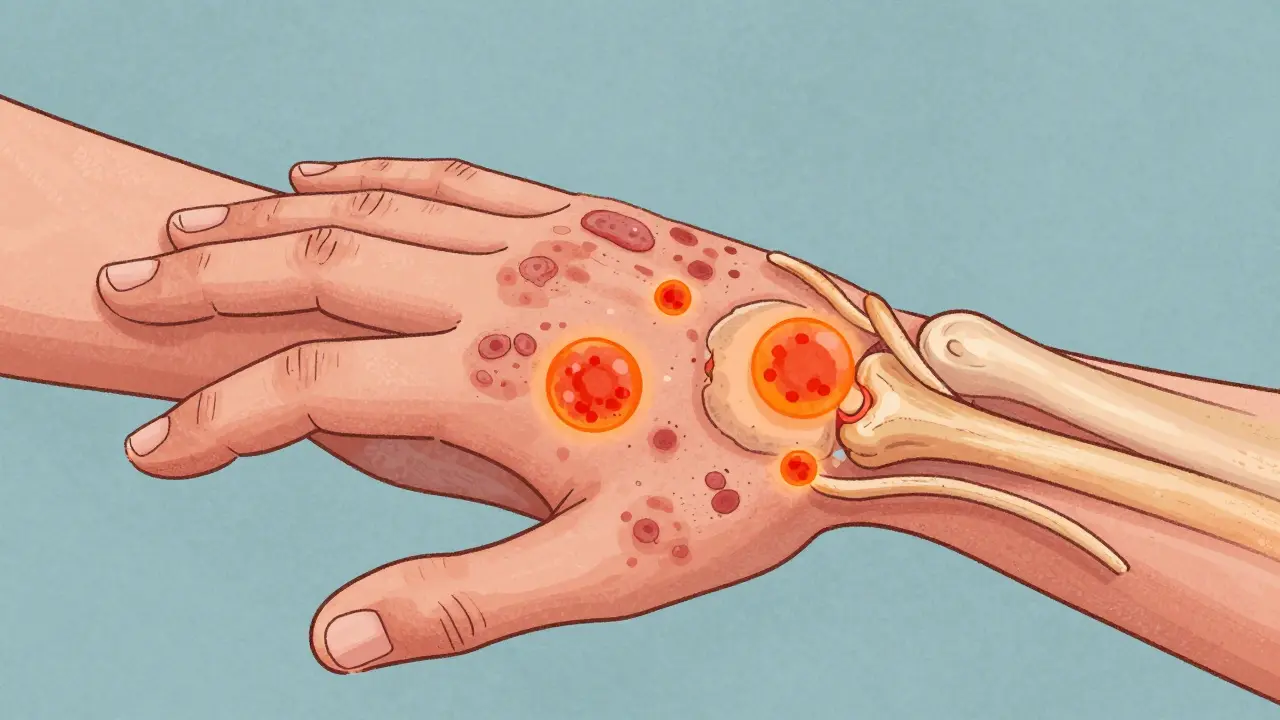
Your skin might be screaming for help with red, scaly patches, but your joints could be suffering in silence. For roughly 30% of people living with psoriasis, a chronic inflammatory skin condition, the battle doesn't end at the surface. It moves deeper, attacking the cartilage and bones, leading to a painful reality known as psoriatic arthritisa chronic autoimmune disease that causes inflammation in the joints and entheses. This isn't just 'old age' wear and tear. It is an aggressive immune system error that can permanently damage your body if you don't catch it early.
You might think arthritis only affects older adults, or that it’s simply the result of using your knees too much. That’s a dangerous myth. Psoriatic arthritis (PsA) is inflammatory. Your immune system, which usually fights off viruses and bacteria, mistakenly targets healthy tissue. It attacks the synovium-the lining of the joints-and the entheses, where tendons and ligaments attach to bone. The result? Swelling, stiffness, and pain that can ruin your quality of life. But here is the good news: understanding exactly what is happening inside your body is the first step toward stopping it.
The Silent Link Between Skin and Joints
Most people assume that if they have psoriasis, they will eventually get PsA, or vice versa. The truth is more nuanced. While about 1-2% of the general population has PsA, the timeline varies wildly. For most, the skin symptoms show up first. You might deal with plaques on your elbows or scalp for five to ten years before your fingers start swelling. However, in about 15% of cases, the joint pain hits before you see a single rash. This makes diagnosis incredibly tricky. Doctors often misdiagnose it as rheumatoid arthritis or osteoarthritis, leaving patients waiting years for proper treatment.
Why does this happen? It comes down to genetics and triggers. If you carry certain genetic markers, like HLA-B27, your risk skyrockets. But genes alone aren’t enough. Something needs to spark the fire. Common triggers include severe stress, physical trauma to a joint, or even a simple strep throat infection. Once the immune system flips the switch, it stays on, creating a cycle of inflammation that damages both your skin barrier and your joint structure.
Recognizing the Five Faces of Psoriatic Arthritis
PsA isn’t one-size-fits-all. It shows up in five distinct patterns, and knowing which one you have helps doctors treat you better. Here is how it typically presents:
- Asymmetric Oligoarthritis: This is the most common form, affecting 35-40% of patients. It hits fewer than five joints, and they are rarely mirrored on both sides of your body. You might have a swollen left knee and a painful right wrist. It’s unpredictable and frustrating.
- Symmetric Polyarthritis: Affecting 25-30% of people, this looks a lot like rheumatoid arthritis. It strikes similar joints on both sides-both hands, both feet. Because it mimics other conditions, it’s often misdiagnosed initially.
- DIP Predominant Arthritis: This type targets the distal interphalangeal joints-the ones closest to your fingernails. It’s unique to PsA; you won’t see this pattern in rheumatoid arthritis. If your fingertips are swollen and your nails are pitted, this is a major clue.
- Spondylarthritis: About 5-10% of patients experience inflammation in the spine and sacroiliac joints. This causes deep lower back pain that gets worse when you rest and improves when you move. It’s not just a stiff back; it’s structural inflammation.
- Arthritis Mutilans: This is the rarest and most severe form, affecting less than 5% of people. It causes rapid bone destruction, leading to shortened fingers-a deformity sometimes called 'opera glass hand.' It’s devastating, but thankfully uncommon with modern treatments.
Beyond the Joints: Dactylitis and Enthesitis
If you only look for joint pain, you’re missing half the story. Two specific symptoms set PsA apart from almost every other type of arthritis.
First, there is dactylitisdiffuse swelling of an entire finger or toe, often called 'sausage digits'. Imagine your whole finger swells up like a sausage. It’s not just the knuckle; it’s the tendon sheath and the joint together. This happens in 40-50% of PsA patients. It’s painful, stiff, and unmistakable. If you wake up and your pinky looks like a hot dog, that’s a red flag.
Second, watch out for enthesitisinflammation at the sites where tendons and ligaments insert into bone. This is inflammation where your Achilles tendon meets your heel, or where your plantar fascia attaches to your foot. It causes sharp, stabbing pain, especially in the morning or after sitting for a long time. Up to 50% of PsA patients suffer from this. It’s why walking barefoot on cold floors can feel like stepping on knives.
| Feature | Psoriatic Arthritis (PsA) | Rheumatoid Arthritis (RA) | Osteoarthritis (OA) |
|---|---|---|---|
| Type | Inflammatory/Autoimmune | Inflammatory/Autoimmune | Degenerative/Wear-and-Tear |
| Joint Pattern | Often asymmetric; affects DIP joints | Symmetric; spares DIP joints | Weight-bearing joints; variable |
| Nail Changes | Common (pitting, separation) | Rare | Absent |
| Blood Test Marker | Rheumatoid Factor Negative | Rheumatoid Factor Positive (80%) | Normal |
| X-Ray Signs | 'Pencil-in-cup' deformity; new bone growth | Joint erosion; no new bone | Narrowed joint space; bone spurs |
| Spine Involvement | Yes (Spondylitis) | No (except neck) | Yes (Degenerative) |

The Diagnostic Trap: Why Early Action Matters
Here is the hard truth: the average person waits 2 to 5 years to get a correct diagnosis for PsA. During that time, irreversible damage is occurring. Bone erosion doesn't wait for paperwork. Studies show that if you delay treatment by more than six months, your risk of permanent joint damage increases significantly. By the time many patients see a rheumatologist, they’ve already visited three or four different doctors who missed the mark.
So, how do you avoid the trap? Look for the cluster. Don’t just report 'joint pain.' Tell your doctor about the nail pitting. Mention the morning stiffness that lasts longer than 30 minutes. Point out the sausage-like swelling in your toes. When nail psoriasis and dactylitis appear together, the specificity for diagnosing PsA jumps to 89%. You are your own best advocate. If your primary care physician dismisses your pain as 'just aging,' seek a second opinion from a rheumatologist immediately.
Treatment Strategies: From DMARDs to Biologics
Gone are the days when doctors just told you to take ibuprofen and live with it. Today’s treatment landscape is robust, aiming for 'minimal disease activity' rather than just symptom relief. The goal is to stop the inflammation before it destroys the joint.
Treatment usually starts with conventional synthetic DMARDsDisease-Modifying Antirheumatic Drugs like methotrexate. Methotrexate is the gold standard starter drug for about 65% of newly diagnosed patients. It slows down the immune system’s attack. But if that isn’t enough, or if you have severe skin involvement, doctors move to biologics.
Biologics are targeted therapies. They block specific proteins involved in inflammation. TNF inhibitors were the first wave, helping millions. Now, we have IL-17 and IL-23 inhibitors. These newer drugs are game-changers. For example, guselkumab, an IL-23 inhibitor, showed a 64% response rate in recent trials. They work faster and often clear the skin completely while calming the joints. About 65% of patients achieve minimal disease activity within six months of starting a TNF inhibitor.
However, it’s not all smooth sailing. About 30% of patients don’t respond well to the first biologic they try. This is why personalized medicine is becoming critical. Doctors are now looking at genomic markers to predict which drug will work for you, sparing you months of trial and error.
Lifestyle Factors: What You Can Control
Medication is powerful, but it’s not magic. Your lifestyle plays a huge role in keeping flares at bay. Stress is the number one trigger reported by patients-85% say it worsens their symptoms. When you’re stressed, your body releases cortisol and other hormones that can exacerbate inflammation. Mindfulness, therapy, or even just regular walks can lower that baseline stress.
Weight management is another non-negotiable factor. Obesity doesn’t just put mechanical stress on your knees; fat tissue itself produces inflammatory chemicals called adipokines. Having a BMI over 30 increases your risk of developing PsA by 2.3 times. Losing weight reduces this chemical load and makes medications work better. Even a modest 5-10% weight loss can improve treatment outcomes significantly.
Don’t forget about smoking and alcohol. Smoking interferes with the effectiveness of methotrexate and increases cardiovascular risk, which is already higher in PsA patients. Alcohol can interact dangerously with liver-metabolized drugs like methotrexate. Cutting back isn’t just good advice; it’s part of your medical regimen.
Living With PsA: Protecting Your Future
Psoriatic arthritis is a marathon, not a sprint. It requires coordination between dermatologists and rheumatologists. Research shows that integrated care models lead to 82% optimal outcomes compared to 54% when specialists work in silos. Make sure your doctors talk to each other.
Keep an eye on your overall health. PsA increases the risk of heart disease and diabetes because systemic inflammation affects blood vessels and insulin sensitivity. Regular check-ups for blood pressure, cholesterol, and blood sugar are essential. Exercise is crucial, but choose low-impact activities like swimming or cycling to protect your joints while staying strong.
The future looks brighter. New clinical trials are exploring JAK inhibitors and novel pathways that could offer even more precise control. But for today, the key is vigilance. Know your body. Track your symptoms. And never accept 'this is normal' as an answer for persistent pain. You deserve to move freely, without fear of the next flare.
Can psoriatic arthritis go away on its own?
No, psoriatic arthritis is a chronic, progressive autoimmune disease. It does not resolve spontaneously. Without treatment, the inflammation continues to damage joints and bones. However, with effective medication, many patients achieve remission, meaning they have no active symptoms and no further progression of damage.
What is the difference between psoriatic arthritis and rheumatoid arthritis?
While both are inflammatory autoimmune diseases, RA typically affects joints symmetrically (both hands/knees) and is associated with positive rheumatoid factor blood tests. PsA often affects joints asymmetrically, involves the spine and fingertips (DIP joints), and is linked to skin/nail psoriasis. PsA also causes unique features like dactylitis ('sausage digits') and enthesitis, which are rare in RA.
How long does it take to get a diagnosis for psoriatic arthritis?
Unfortunately, the average diagnostic delay is 2 to 5 years. This is because symptoms can be intermittent and mimic other conditions. Early signs like nail pitting and morning stiffness are often overlooked. Seeing a rheumatologist early and providing a detailed history of skin issues can speed up this process significantly.
Does diet affect psoriatic arthritis?
Yes, indirectly. An anti-inflammatory diet rich in omega-3 fatty acids (found in fish), fruits, vegetables, and whole grains can help reduce systemic inflammation. Conversely, high sugar, processed foods, and excessive alcohol can trigger flares. Weight loss through diet is particularly beneficial as fat tissue produces inflammatory cytokines.
Are biologics safe for long-term use?
Biologics are generally safe and highly effective for long-term management. They do carry risks, such as increased susceptibility to infections, so doctors screen for tuberculosis and hepatitis before starting. Some newer classes, like JAK inhibitors, have specific warnings regarding cardiovascular health. Regular monitoring ensures safety while maximizing benefits.

