That sharp, stabbing pain when you reach for a coffee mug or try to scratch your back is more than just an annoyance-it’s a signal that something is wrong with your shoulder mechanics. For millions of people, this discomfort stems from two closely linked conditions: rotator cuff injuries, which involve damage to the tendons stabilizing the joint, and subacromial bursitis, inflammation of the fluid-filled sac that cushions those tendons. While these terms sound complex, the reality is often simple: friction. When the bones and soft tissues in your shoulder don’t glide smoothly, pain follows. The good news? You likely do not need surgery. Most cases resolve with targeted rehabilitation and smart lifestyle adjustments.
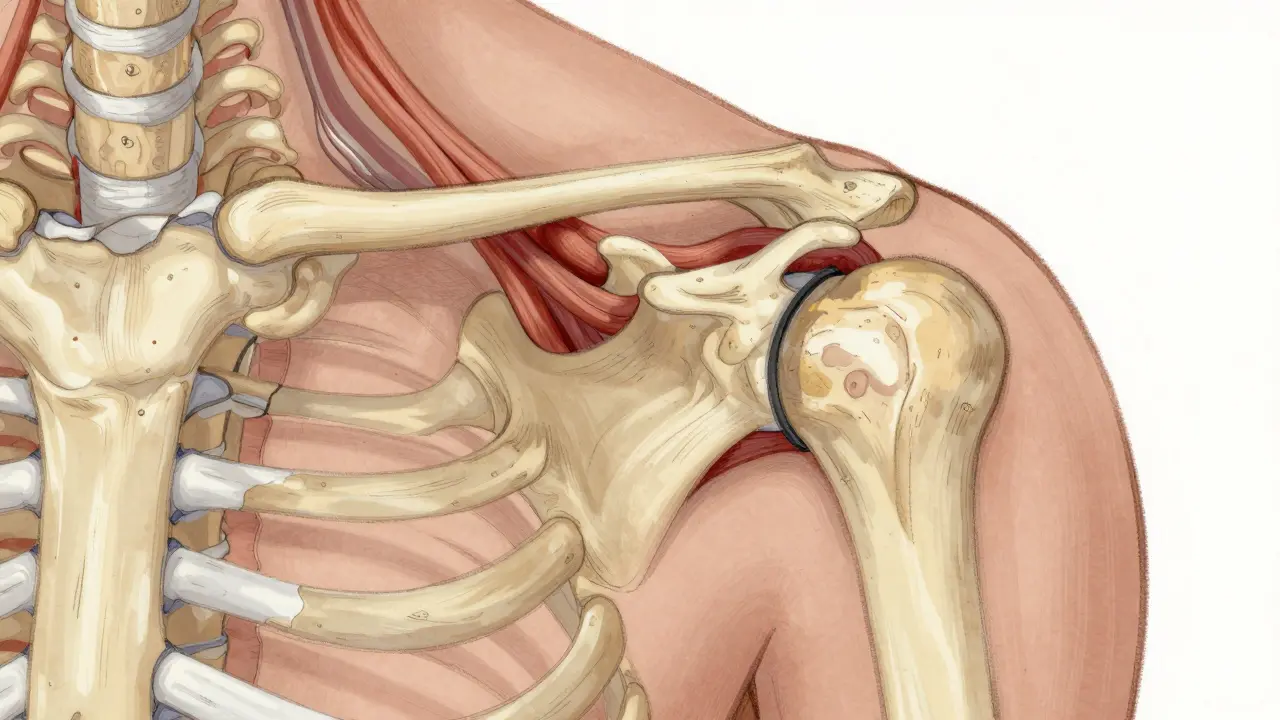
Understanding why this happens is the first step toward fixing it. Your shoulder is the most mobile joint in the human body, but that mobility comes at the cost of stability. It relies on four small muscles-the supraspinatus, infraspinatus, teres minor, and subscapularis-known collectively as the rotator cuff. These muscles keep the ball of your upper arm bone centered in the shallow socket of your shoulder blade. Above them sits the acromion, a bony arch. Between the rotator cuff tendons and the acromion lies the subacromial bursa, a thin sac filled with lubricating fluid. When you lift your arm, these structures must pass each other without touching. If they rub, you get impingement. This friction causes the bursa to swell (bursitis) and the tendons to fray or tear (rotator cuff injury).
Identifying the Source of Your Shoulder Pain
Not all shoulder pain is created equal, but rotator cuff issues and bursitis share a distinct signature. The most common clue is the "painful arc." Try raising your arm out to the side. If it hurts specifically between 60 and 120 degrees of elevation, but feels fine at the bottom and top, you are likely experiencing subacromial impingement. This happens because that specific range of motion is where the space between the acromion and the rotator cuff is narrowest.
Nighttime pain is another major red flag. Many patients report being unable to sleep on the affected side because the weight of the arm compresses the inflamed bursa against the bone. The pain is often described as a dull, deep ache rather than a sharp sting, though sudden movements can trigger acute spikes. If you have recently started a new exercise routine involving overhead presses or swimming, or if your job requires repetitive lifting above shoulder height, you are in the high-risk group. Construction workers, for instance, face a 32% higher incidence of these injuries compared to the general population due to constant overhead strain.
Diagnosis usually starts with a physical exam. A doctor will check your range of motion and strength. If symptoms persist, imaging becomes necessary. Ultrasound is excellent for detecting bursal thickening; anything over 2 mm is considered abnormal. MRI provides a more detailed view, showing whether there is fluid in the bursa (indicating active inflammation) or if the tendon has partially or completely torn. Knowing the difference matters because a complete tear in someone over 60 may require different management than simple inflammation in a 30-year-old athlete.
Why Surgery Is Rarely the First Option
It is natural to want a quick fix, and surgery sounds definitive. However, current medical consensus strongly favors conservative care. Approximately 80% of rotator cuff tendinitis and bursitis cases improve significantly with non-surgical treatment. Surgery, such as arthroscopic subacromial decompression, involves shaving down the acromion bone to create more room for the tendons. While effective for some, recent studies show no significant difference in long-term outcomes between surgery and intensive physical therapy for isolated bursitis or small tears.
Consider the trade-offs. Surgery costs between $15,000 and $20,000 and carries risks like infection or stiffness. Recovery takes months, during which you cannot use the arm normally. Conservative management, by contrast, costs a fraction of that amount and preserves your native anatomy. The downside is time and discipline. It requires 8 to 12 weeks of consistent effort. But for most people, avoiding the operating table is worth the wait. Surgery is typically reserved for cases where pain persists after six months of dedicated rehabilitation or for massive, traumatic tears in younger, active individuals.

The Role of Injections and Medication
In the early stages, reducing inflammation is key to breaking the pain cycle. Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can help manage pain and swelling. Take them as directed, usually 400-600 mg three times daily, but be mindful of stomach irritation. Ice is also crucial. Apply ice packs for 15-20 minutes, three to four times a day, especially after activity. This constricts blood vessels and reduces the inflammatory response.
If oral medications and rest do not provide relief within four to six weeks, a corticosteroid injection may be recommended. This involves injecting a mix of steroid (like triamcinolone) and local anesthetic directly into the subacromial space under ultrasound guidance. This procedure provides significant pain relief in 65-75% of patients, lasting anywhere from four to twelve weeks. This window of reduced pain is critical because it allows you to participate fully in physical therapy without guarding against movement.
However, injections are not a cure-all. They should be limited to two or three per year. Frequent steroid use can weaken tendons, increasing the risk of rupture. Newer alternatives like platelet-rich plasma (PRP) injections are gaining traction. PRP involves drawing your own blood, concentrating the healing factors, and injecting them back into the shoulder. Early data suggests a 68% success rate for stubborn cases, making it a promising second-line option if steroids fail.
Effective Rehabilitation Exercises
Physical therapy is the cornerstone of recovery. The goal is not just to strengthen the rotator cuff but to stabilize the scapula (shoulder blade). If your shoulder blade doesn’t move correctly, the rotator cuff gets pinched every time you lift your arm. Here is a structured approach to rebuilding shoulder health:
- Pendulum Exercises (Weeks 1-2): Lean forward, letting your affected arm hang loose. Gently swing your arm in small circles using your body momentum, not your shoulder muscles. Do this for 5-10 minutes, three times a day. This maintains mobility without stressing the inflamed tissues.
- Scapular Retractions (Weeks 2-4): Sit or stand tall. Squeeze your shoulder blades together as if trying to hold a pencil between them. Hold for five seconds, then release. Perform three sets of 15 repetitions daily. Strong scapular stabilizers prevent the shoulder from hiking up and narrowing the subacromial space.
- External Rotation with Resistance Band (Weeks 4-6): Attach a resistance band to a doorknob. Keep your elbow tucked into your side at a 90-degree angle. Rotate your forearm outward away from your body. Use light resistance (30-50% of max effort). Do 15-20 reps. This strengthens the infraspinatus and teres minor, key stabilizers.
- Wall Slides (Weeks 6+): Stand with your back against a wall. Raise your arms to a "goalpost" position (elbows bent at 90 degrees). Slowly slide your hands up the wall while keeping your elbows and wrists in contact with the surface. This promotes full overhead mobility safely.
Consistency beats intensity. Doing these exercises gently every day is far more effective than pushing through pain once a week. Monitor your pain on a scale of 0-10. If an exercise pushes pain above a 5, stop or reduce the resistance. Mild discomfort is normal; sharp pain is not.

Lifestyle Adjustments for Long-Term Relief
Rehabilitation isn't just about the exercises you do in the gym; it's about how you move throughout the day. Poor posture is a silent enemy of shoulder health. Slouching at a desk rounds the shoulders forward, compressing the front of the joint and narrowing the space for the rotator cuff. Make sure your workstation is ergonomic: keep your monitor at eye level and your elbows supported at 90 degrees.
Sleep position matters too. Avoid sleeping on the injured side. If you sleep on your back, place a pillow under the affected arm to keep it slightly elevated and supported. This prevents the humerus from dropping back and stretching the inflamed tissues overnight. For side sleepers, hug a pillow to keep the top arm from collapsing across your chest.
Return to sport or heavy labor gradually. The "weekend warrior" syndrome is real. Patients who rush back to tennis or construction work after feeling better often relapse. Increase activity levels by no more than 10% per week. Listen to your body. If pain returns after activity, you have progressed too quickly. Step back, ice, and resume only when pain-free.
| Treatment Method | Time to Relief | Success Rate | Risks/Costs |
|---|---|---|---|
| Conservative Care (PT + NSAIDs) | 8-12 weeks | ~80% | Low risk, low cost ($1,500-$3,000) |
| Corticosteroid Injection | 4-12 weeks (temporary) | 65-75% short-term relief | Tendon weakening if overused |
| Arthroscopic Surgery | 4-6 months recovery | Variable (no clear advantage over PT for bursitis) | High cost ($15k-$20k), surgical risks |
| PRP Injection | 3-6 months | ~68% in resistant cases | Moderate cost, minimal risk |
When to Seek Immediate Medical Attention
While most shoulder pain is mechanical and manageable, certain signs indicate a more serious problem. Seek immediate care if you experience:
- Sudden inability to lift the arm: This could indicate a massive rotator cuff tear.
- Visible deformity: A bump near the shoulder tip might suggest a dislocation or fracture.
- Severe night pain unrelieved by medication: This can sometimes indicate referred pain from heart or gallbladder issues, though less common.
- Fever or redness: Signs of infection in the joint, which is a medical emergency.
For typical rotator cuff and bursitis issues, patience is your best ally. The shoulder is resilient. With the right combination of anti-inflammatory measures, targeted strengthening, and postural awareness, you can restore full function and get back to your life without enduring unnecessary procedures.
How long does it take for shoulder bursitis to heal?
Most cases of subacromial bursitis improve within 8 to 12 weeks with consistent physical therapy and activity modification. Some patients experience relief sooner with corticosteroid injections, but full functional recovery typically requires completing a structured rehab program.
Can rotator cuff tears heal without surgery?
Yes, many partial tears and even some full-thickness tears can be managed successfully without surgery, especially in older adults. Studies show that 80% of patients respond well to non-surgical treatments like physical therapy and injections. Surgery is generally reserved for young athletes or those with massive tears who fail conservative care.
What is the painful arc test?
The painful arc test involves raising your arm out to the side. If you feel pain specifically between 60 and 120 degrees of elevation, but not below 60 or above 120, it suggests subacromial impingement. This occurs because the space for the rotator cuff is narrowest in that middle range of motion.
Are corticosteroid injections safe for shoulder pain?
Corticosteroid injections are generally safe when used sparingly. They provide significant short-term pain relief in 65-75% of patients. However, they should be limited to 2-3 per year to avoid weakening the tendon tissue, which increases the risk of rupture. Always ensure injections are guided by ultrasound for accuracy.
Which exercises are best for rotator cuff rehabilitation?
Key exercises include pendulum swings for early mobility, scapular retractions to stabilize the shoulder blade, and external rotation with resistance bands to strengthen the rotator cuff muscles. Consistency is more important than intensity; perform these exercises daily with light resistance to avoid aggravating the injury.
Does sleeping position affect shoulder pain?
Yes, sleeping on the affected side can compress the inflamed bursa and worsen pain. Sleeping on your back with a pillow under the arm or hugging a pillow if on your other side helps maintain proper alignment and reduces pressure on the shoulder joint overnight.

